Circulation
Pulses
Pulses can be palpated on all four of Paul‘s extremities, both brachial pulses and both femoral pulses.
When an umbilical cord is present, an umbilical cord pulse can be palpated at the 12 o’clock position just above the cord, under the skin.
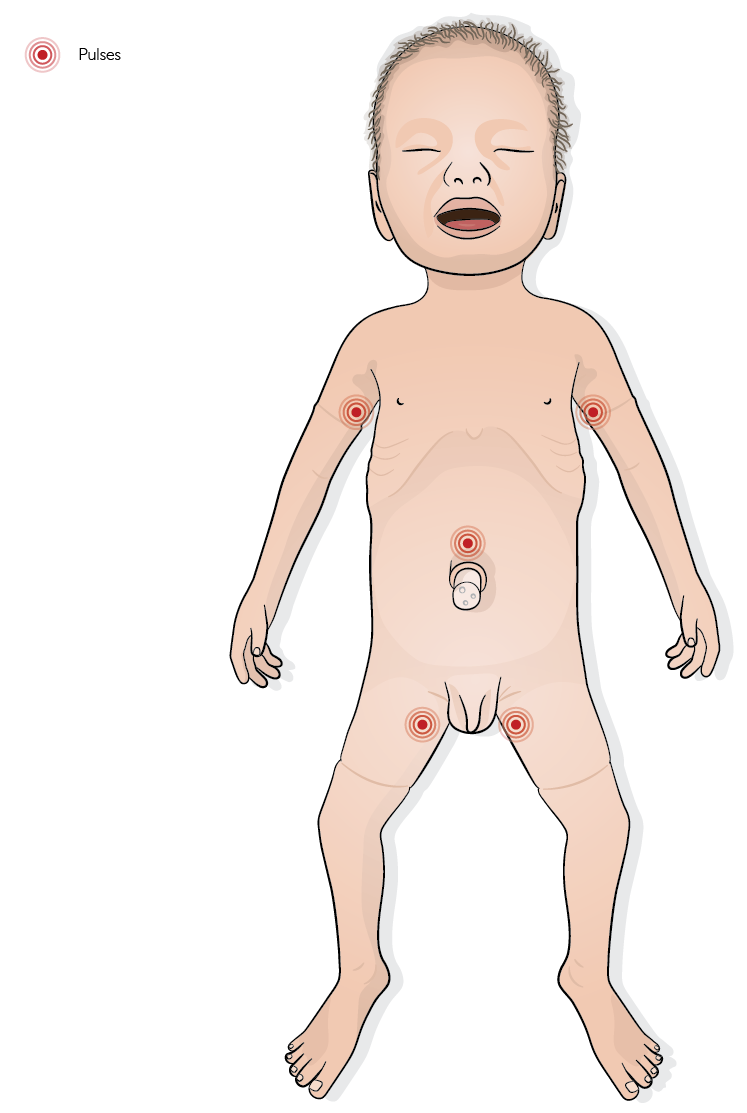 |
The pulses can be switched on and off individually using the bubbles in the upper arm and femoral area.
A yellow bubble indicates an active pulse.
A red bubble indicates a switched-off pulse.
The intensity of the pulse can also be changed in the pre-sets.
 |
NOTE
For more information, refer to the Pre-sets section.
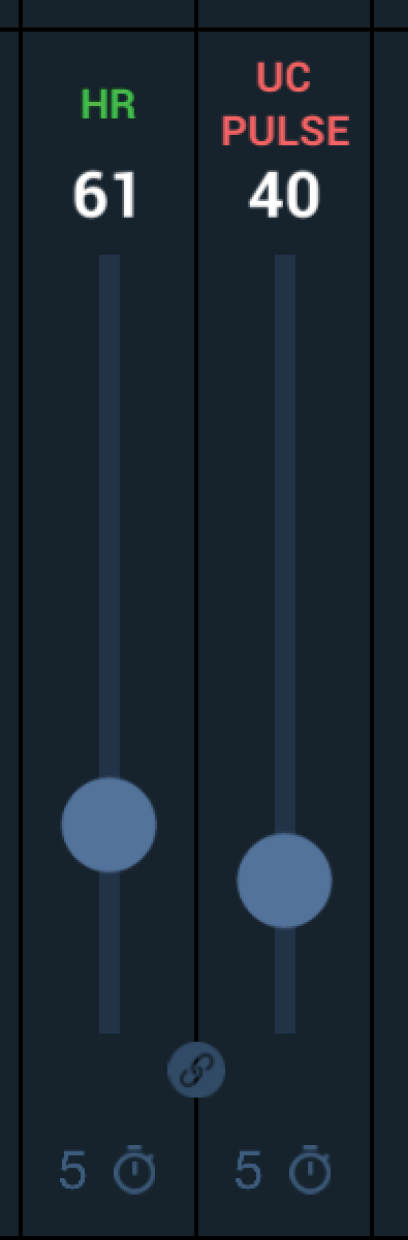
Umbilical cord pulse
In postnatal scenarios with an umbilical cord attached to the simulator, an umbilical cord pulse can be felt. If Paul is postnatally in a state of massive circulatory insufficiency (heart rate < 60/min), the umbilical cord pulse can be decoupled from the heart rate and a lower pulse (or a non-palpable pulse) can be set on the umbilical cord than indicated by the heart rate in the sense of a pulse deficit.
 |
Capillary refill time
Paul can simulate a capillary refill time (CRT), allowing trainees to assess circulatory status.
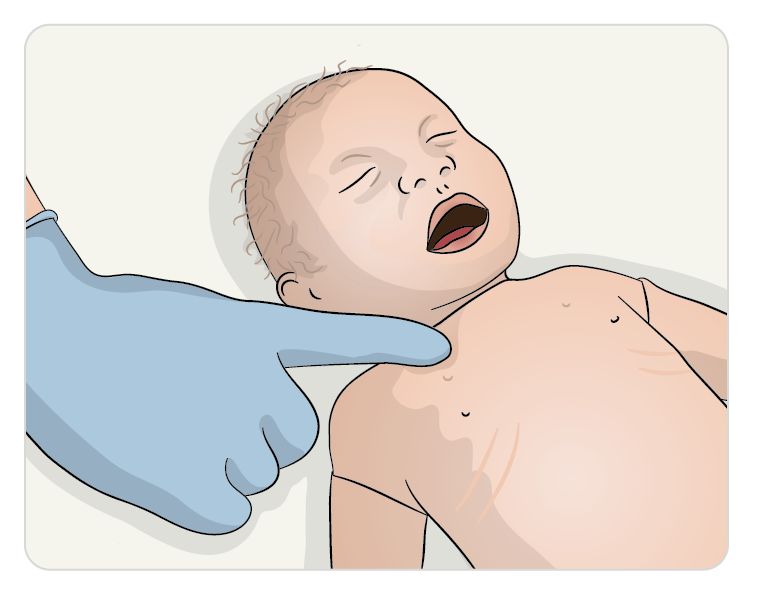
The desired refill time can be freely selected via a control window in Paul 3D simulation.
On the simulator, the test area is located at the right clavicle (collarbone).
When pressing in this area, an LED indicates the set refill time, simulating the return of color.
The test time and measured refill time are automatically recorded and transferred to the debriefing system for later review.
Chest compression
Chest compressions can be performed on Paul with a realistic impression depth (approx. 1/3 of the thorax diameter).
 |
During chest compressions, hands appear on the 3D animation to indicate that chest compressions are being performed.
When chest compressions are performed, a window displays the effectiveness of chest compressions and ventilations.
By clicking the small plus (+) icon in the chest compression window, additional details can be displayed, including compression rate and percentage of effective chest compressions.
When chest compressions and ventilations are performed in alternation, this area also displays the effectiveness of ventilations and the compression-to-ventilation ratio.
NOTE
The display window can be shown or hidden as required.
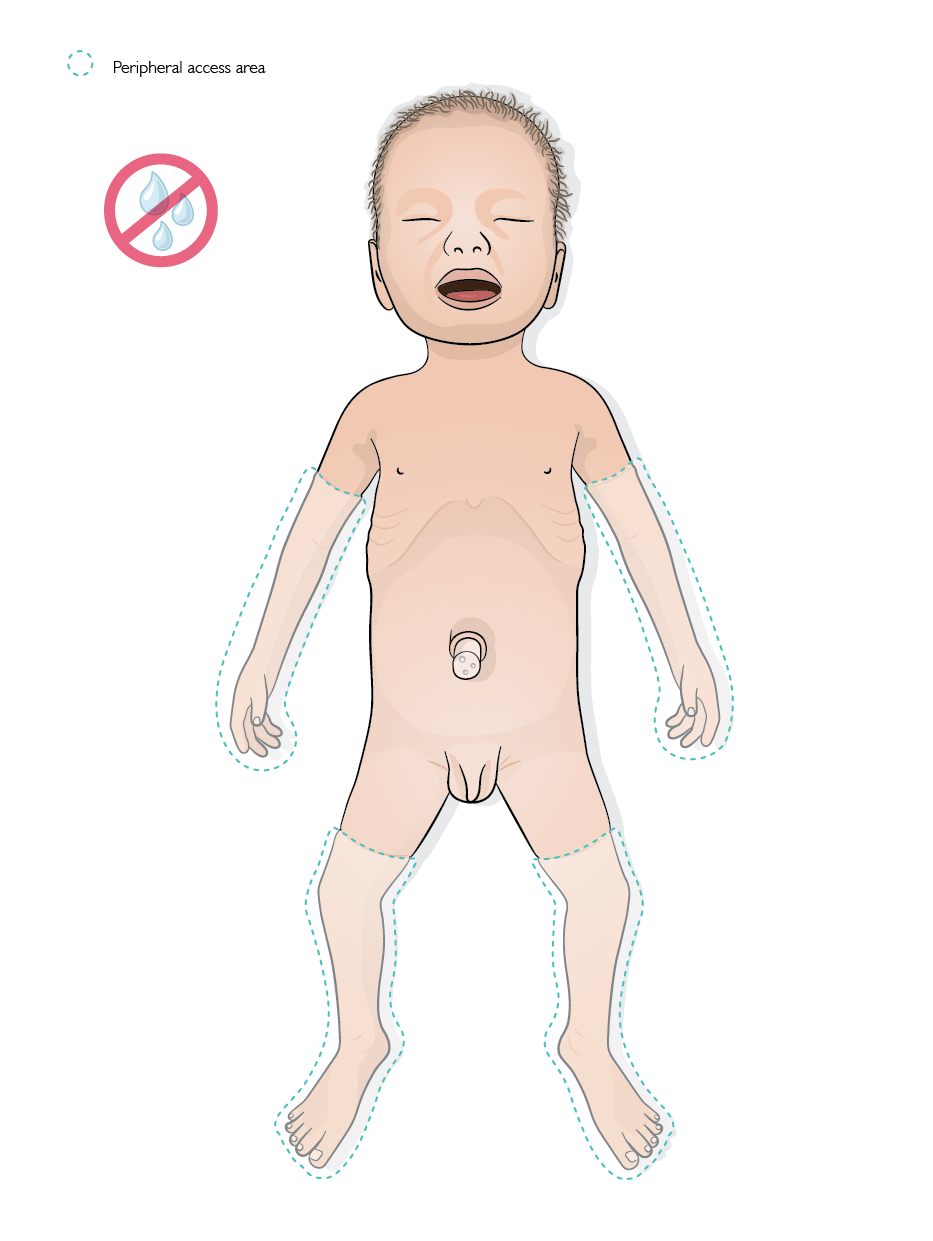
Peripheral access
Peripheral accesses (24GA or 26GA) can be inserted into all of Paul‘s extremities. Paul‘s silicone skin closes up after the access is removed. If necessary, all four extremities can be easily replaced.
 |
CAUTIONS
Peripheral accesses must never be placed in Paul‘s head or neck area. This can lead to serious damage to the technology incorporated in these areas.
Do not inject drugs or fluids into the peripheral accesses in Paul as this can damage de simulator. Use a bag system with a three-way stopcock for a realistic injection of drugs and fluids. For more information, refer to the Administrating drugs and fluids section.
TIPS
Training participants must be informed that they will have to puncture a little deeper under Paul‘s skin than usual when inserting a peripheral access, as the plastic cannula of the indwelling venous cannula is rather difficult to push under the silicone skin.
Plaster strips for vascular access fixation, such as Steri-Strips®, do not adhere well to silicone simulators like Paul. We therefore recommend that you first apply a strip of silicone plaster (e.g. Mepitac®) to the areas of skin where the Steri-Strips® will ultimately be attached. The plaster strip can then be firmly attached to it.
Cardioversion and defibrillation with Shocklink
Paul supports cardioversion and defibrillation training through the Laerdal ShockLink® system.
Although shockable rhythms are extremely rare in the neonatal period, defibrillation may be required in specific cases - for example, in children with congenital heart defects.
Slightly more common, though still rare, is the potential need for cardioversion, such as in cases of supraventricular tachycardia (SVT).
While these conditions are not the primary focus of a neonatal simulator, Paul is capable of simulating shockable rhythms and can be cardioverted or defibrillated using the Laerdal ShockLink®.
CAUTION
Never use a real defibrillator directly on Paul. Doing so can cause severe and irreversible damage to the simulator. Always use the Laerdal ShockLink® for cardioversion or defibrillation scenarios.
NOTE
Currently, the ShockLink function is not integrated into the user interface. This feature - allowing direct control of the ShockLink® and defibrillation from within the user interface - will be available as part of a future software update.